
May 15, 2026
The Hidden Mental Health Crisis of Endometriosis
Endometriosis is not just a pain condition.
It is a psychological one.
The part we do not talk about enough
When endometriosis enters clinical and public conversation, the focus tends to land in predictable places. Pain. Fertility. Surgical intervention. These are important. They are not the whole picture.
What the data consistently shows, and what those of us working in health-related quality of life research know intimately, is that the psychological burden of endometriosis is profound, persistent, and largely unaddressed in standard care pathways.
This is not a secondary concern. It is a central one.
What the evidence actually tells us
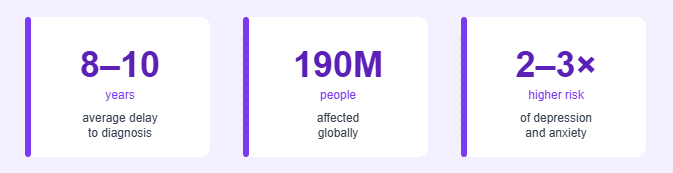
Research places the risk of depression in people with endometriosis at two to three times that of the general population. Anxiety disorders are frequently co-occurring. Post-traumatic stress responses have been documented in relation to clinical encounters alone, not just the disease itself.
This matters because it is not incidental. Chronic pain changes the brain. It sensitises the nervous system, disrupts sleep architecture, and erodes the capacity to regulate mood and stress. These are neurobiological processes, not psychological weakness.
Documented psychological impacts
Significantly elevated rates of depression, particularly correlated with pain severity and diagnostic delay
Anxiety disorders frequently co-occurring, often sustained by medical uncertainty and repeated dismissal
PTSD symptomology linked to traumatic clinical encounters and diagnostic disbelief
Disordered sleep affecting mood regulation, cognitive function, and pain tolerance
Social withdrawal and relationship deterioration as participation in daily life becomes increasingly limited
Career disruption, financial instability, and the grief of lost professional identity
The statistic that should stop us in our tracks
Research by Were, Richardson, and Hughes (2020) found that 60% of women with endometriosis surveyed had either thought about or taken action to end their own lives.
Read that again.
Sixty percent.
This is not a footnote. This is not a peripheral finding. This is a public health crisis sitting inside a condition that is still routinely dismissed, underfunded, and misunderstood. If 60% of people with any other chronic condition reported suicidal ideation or behaviour, it would dominate clinical guidelines, commissioning decisions, and research funding priorities.
For endometriosis, it barely registers in mainstream discourse.
60% of women with endometriosis surveyed had either thought about or taken action to end their own lives.
Were, S., Richardson, T., & Hughes, J. (2020). The Role of Psychological Therapy in Improving the Mental Health of Women with Endometriosis: An Exploratory Study. Solent NHS Trust Research and Improvement Virtual Conference.
The diagnostic delay is not a passive statistic
The 8 to 10 year average delay to diagnosis is cited so often that it risks becoming wallpaper. It should not.
That figure represents years spent being told that pain is normal. Those symptoms are exaggerated. That nothing is wrong. It represents the cumulative psychological cost of medical gaslighting, of learning to distrust your own body because the systems around you consistently failed to validate it.
When pain is dismissed for long enough, people stop trusting their own experience of it. That erosion does not resolve with a diagnosis.
As researchers, we quantify health-related quality of life. As advocates, we witness it. And as patients, many of us live it. The gap between those three vantage points is where so much of the psychological harm accumulates.
Grief that has no clinical category
One of the least examined dimensions of endometriosis is grief. It is real, layered, and rarely acknowledged in clinical settings.
Grief for the person you were before chronic pain became your baseline. Grief for fertility lost or complicated. Grief for the career trajectory that a flare ended. Grief for the relationships that did not survive an invisible illness. These losses do not appear on symptom checklists. They accumulate quietly, across years, largely unwitnessed.
This is not a soft concern. Loss of identity, purpose, and relational connection are established predictors of poor mental health outcomes. We need to name them as such within endometriosis care.
What integrated care actually requires
There is a growing evidence base for multidisciplinary approaches to endometriosis that embed psychological support from the point of diagnosis, not as a referral at the end of a pathway that has already caused harm.
This means pain psychologists are standard within specialist services. Trauma-informed consultation as a baseline competency, not an optional extra. Routine screening for depression and anxiety embedded into care, not bolted on.
It also means the language we use in clinical and advocacy spaces. When endometriosis is framed primarily around fertility outcomes, we erase the significant portion of patients for whom fertility is not the central concern. When we lead with pain scales, we may miss the person who has stopped describing their experience because no one has ever responded to it adequately.
A note on who sustains this work
It is worth stating plainly: much of the advocacy, research communication, and community support around endometriosis is carried by chronically ill people, operating beyond sustainable capacity, in systems that were not designed to accommodate them.
The mental health impact of the condition does not stop at patients. It runs through every layer of this ecosystem. And that is a structural problem, not an individual one.
Sustainable progress requires acknowledging that the people driving change in this space are often unwell themselves. It requires material support of charities and researchers, not just symbolic amplification. And it requires that we build care systems robust enough that they do not depend on patient-advocates running on empty.
If you are struggling
Support is available. You do not have to manage this alone.
Endometriosis South Coast Support groups
Samaritans
Free, confidential support, 24 hours a day, 365 days a year.
Call 116 123 · jo@samaritans.org
Crisis Text Line (Shout) in collaboration with EndoBuddies
Free, confidential crisis support by text, available 24/7.
Text ENDO to 85258
Mind
Mental health information, support, and local services across England and Wales.
0300 123 3393 · mind.org.uk
NHS Urgent Mental Health Support
If you are in crisis, contact your local NHS urgent mental health line or go to your nearest A&E.
111 (select mental health option)